neuroplex
New York Association of Neuropathologists
5/13/2008 Case 4: High grade astroblastoma
Presented by: Dr. Mary Fowkes - Mt. Sinai Hospital
Clinical History:
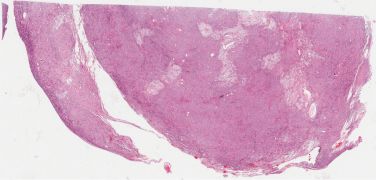
This 23 year old woman had a partial seizure while 36 weeks pregnant. MRI showed a left frontoparietal mass with calcified and cystic areas with enhancement of the soft tissue component, producing edema and mass effect. The mass was resected after the patient was delivered.
Sections showed a small cell neoplasm with calcification, sclerotic vessels and cyst formation, which infiltrated adjacent brain. There were very hyalinized and mineralized regions. Mitotic count was 2/10 HPF. The tumor was positive for vimentin, GFAP, and EMA and a few cells stained for NSE. The tumor was negative for NeuN. MIB1 was 50%.
Diagnostic Notes:
The differential diagnosis included pineal tumor/pineocytoma, meningioma, oligodendroglioma, pilocytic astrocytoma, neuroendocrine neoplasm, glioneuronal tumor and ependymoma. The diagnosis is high grade astroblastoma, on the basis of the immunostaining pattern, which is a new entity in the WHO classification and which does not carry a WHO grade at this time (see Reference). This rare tumor occurs predominantly in children and young adults (median age 11 y; range 1-58 y). Its pattern of broad processes extending to sclerosing blood vessels is characteristic and the tumor is positive for vimentin, S100 and GFAP. MRI findings are important and show a well demarcated, lobulated and calcified enhancing mass. MIB1 is variable. The tumors with low-grade histology have a better prognosis than the high-grade tumors.
References:
-
Aldape KD, Rosenblum MK. Astroblastoma, In: WHO Classification of tumors of the central nervous system, IARP, Lyon, 2007, pp. 88-89.