neuroplex
New York Association of Neuropathologists
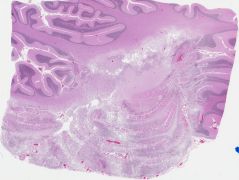
8/12/2008 Case 1: Malacoplakia in brain infarcts
Presented by: Dr. Roy Rhodes - Robert Wood Johnson University Hospital
Clinical History:
A 73-year-old woman with diabetes mellitus, systemic hypertension, hyperparathyroidism, and end-stage renal failure for which she was receiving peritoneal dialysis was treated for peritonitis at another hospital three weeks prior to admission, initially having presented with headache, confusion, agitation and intermittent aggressive behavior. Following admission for increasing confusion, agitation and a gait disturbance, MRI on hospital day 5 revealed an acute left cerebellar infarct in the territory of the posterior inferior cerebellar artery. CT of the cerebellum on day 15 revealed less edema and diminished mass effect. A small acute right occipital infarct was found by MRI on day 16. She had growth of enterococcal species and Klebsiella pneumoniae from peritoneal fluid, and Candida albicans was cultured from blood. A splenic abscess was drained with coagulase-negative staphylococcal species isolated, and antibiotic and antifungal treatment was given. A fluctuating mental status was thought to be based on medications, infections and cerebral ischemia. There were reportedly no cognitive problems prior to the initial episode (per her husband). Serum calcium was 10.9 mg/dl (reference range, 8.5–10.5 mg/dl) and phosphate was 9.4 mg/dl (2.7–4.6 mg/dl). She deteriorated and expired six weeks after admission.
Autopsy showed arterial and venous thromboembolism. The brain weighted 1155 grams, had a right occipital infarct and a soft left lateral cerebellum, which showed liquefactive necrosis, dystrophic calcification, and well-defined round fungus-like bodies. The bodies are Michaelis-Gutman bodies.
Diagnostic Notes:
The diagnosis was malakoplakia.
Malakoplakia usually occurs in the urinary tract. The Michaelis-Gutman bodies are both extra- and intra-cellular and represent incompletely digested bacteria. The lysosomes cannot completely digest the bacteria, and the residua produce a target-like appearance on light microscopy. On electron microscopy, hydroxyapatite crystals are seen which contain calcium, phosphate, iron and carbohydrate and have the appearance of thin needle-like structures as shown by Dr. Rhodes, whose ultramicrographs also showed possible bacteria. The above minerals and carbohydrate are deposited upon incompletely digested bacteria leading to the appearance of Michaelis-Gutman bodies. Malakoplakia of the CNS has been reported in both children and adults. Three previous cases of renal failure all had lesions in the cerebrum, not the cerebellum as in the current case. In AIDS, malakoplakia lesions show intracellular coccobacilli.