neuroplex
New York Association of Neuropathologists
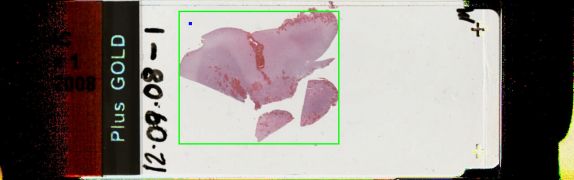
12/9/2008 Case 1: Amyloidosis in the choroid plexus
Presented by: Dr. Crary - Columbia-Presbyterian
Clinical History:
A 72-year-old woman with diabetes mellitus, systemic hypertension, hypertension, congestive heart failure (diastolic dysfunction), end-stage renal disease and renal transplantation (1/2001), was admitted on 7/28/08 for abdominal pain and shortness of breath requiring intubation. She subsequently developed multiple problems including diarrhea due to Strongyloides, disseminated intravascular coagulation and a pseudomonas urinary tract infection. She had altered mental status, but a CT scan was unremarkable except for mild hydrocephalus; there was no acute abnormality. MRI showed a cerebellar lesion thought to represent subacute hemorrhage, and slight atrophy; there was opacification of the mastoid and middle ear. The patient expired on 9/27/08.
The slides showed choroid plexus with amorphous eosinophilic material, metaplastic lamellar bone and calcification.
Diagnostic Notes:
The diagnosis was amyloidosis in the choroid plexus.
Pertinent previous history: In 1989 at age 53, the patient presented with lower back pain and nephrotic syndrome with proteinuria for several years. There was pedal edema. Renal biopsy showed amyloid in the interstitium which was positive for lambda light chains. SEP and UPEP were negative throughout the course and bone marrow biopsy was equivocal. The diagnosis was amyloidosis of the AL type. Dialysis was begun in 1994 and renal transplant took place in 2001.
Autopsy revealed marked amyloid deposition in the native kidney and the transplant and in the heart, where fibrosis was also present. Numerous plasma cells were present in the bone marrow. The brain was grossly unremarkable except for a large pineal gland. Amyloid was found in the anterior and posterior pituitary gland, median eminence and pineal, all regions without a blood-brain barrier. Other areas without a blood brain barrier include the subfornical organ, subcommissural organ (some discussion ensued about whether or not the two latter locations are present in humans), infundibulum, the organum vasculosum of the lamina terminalis, and the area postrema of the medulla.
References:
- Schroder R, Linke RP. Cerebrovascular involvement in systemic AA and AL amyloidosis: a clear haematogenic pattern. Virch Arch 1999;434:551-60.
- Haan J, Roos RA. Amyloid in central nervous system disease. Clin Neurol Neurosurg 1990;92(4):305-10.