neuroplex
New York Association of Neuropathologists
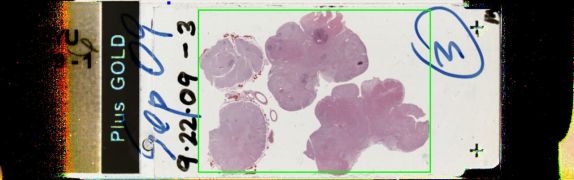
9/22/2009 Case 3: Bilateral inferior olivary hypertrophy, Global hypoxic-ischemic encephalopathy
Presented by: Dr. Irina Mikolaenko and fellows - New York University Medical Center
Clinical History:
The patient is a 59 year old Asian male with a past medical history of hypertension, diabetes, chronic obstructive pulmonary disease, atrial fibrillation, pulmonary embolism and congestive heart failure with ejection fraction of 15-20%. The patient had a history of a cerebrovascular accident in 8/08 with resulting aphasia, left hemiplegia and persistent vegetative state with ventilator dependence. MRI showed remote bilateral middle cerebral artery infarcts, moderate microvascular disease, and stable moderate ventricular enlargement. The patient lived in a nursing home. He declined and died in 6/2009.
The 1100 gram brain showed multiple infarcts, with attenuated white matter and cortex. There cerebellum contain infarcts and the dentate nucleus showed marked neuronal loss, with perineuronal vacuolation, and vacuoles in the remaining neurons. There was hippocampal sclerosis. A section of medulla showed hypertrophy of the inferior olivary nucleus.
Diagnostic Notes:
The proffered diagnoses were respirator brain and inferior olivary hypertrophy. Discussion centered on the findings that characterize respirator brain, and the anatomy and neurophysiology of (pseudo)hypertrophy of the inferior olivary nuclei.
Respirator brain is also known as "non-perfused brain" or "permanent global ischemia." In such cases, mean arterial blood pressure is lower than intracranial pressure, resulting in failure of perfusion of the brain. The brain is dusky brown, soft, friable and eventually liquefied. Landmarks and previous lesions are difficult or impossible to identify. The present case is better termed "hypoxic-ischemic encephalopathy, chronic, diffuse" because it does not show the above mentioned features of respirator brain.
Olivary (pseudo)hypertrophy results after a lesion in the dentatorubro-olivary pathway, and palatal myoclonus is the clinical correlate. A pathological study of several cases using immunohistochemical methods and an antibody against alpha-B-crystallin, heat shock protein and others, suggested that stress produced hypertrophic neurites and demonstrated altered connectivity.
References:
- Katsuhiko Ogawa, Tomohiko Mizutani, Kenji Uehara, Masayuki Minami, Yoshio Suzuki, Toshiki Uchihara. Pathological study of pseudohypertrophy of the inferior olivary nucleus. Neuropathology 2009; doi:10.1111/j.1440-1789.2009-01033.x